We have no clinical information about this patient, except that he was complaining of chest pain, and was initially treated by prehospital paramedics.
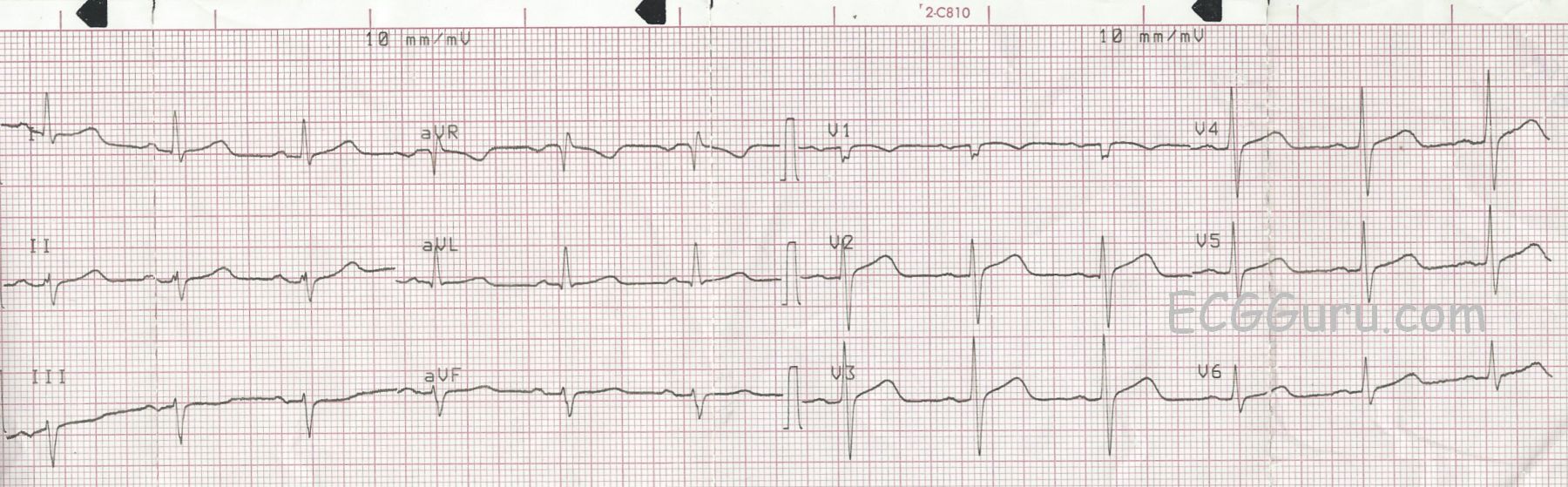
ST Changes The paramedics noted a slight J point elevation in the precordial leads, specifically about one mm of elevation in Leads V2, V3, and V4. In addition, the ST segments are curved downward like a frown in V1 and straight in the remaining precordial leads. Because of the patient’s symptoms, and the ST abnormalities, they notified the hospital that they believed this was a STEMI. The patient was transported without complications, and the Emergency Department physician subsequently downgraded the initial assessment of STEMI Alert. We do not have access to follow up. These ST segments are abnormal, but do not necessarily indicate an acute ST-elevation M.I. (STEMI). A flat or “frowning” ST segment DOES suggest coronary artery disease, and the patient’s symptoms are worrisome. However, before activating the cath lab emergently, it is sometimes preferable to observe the patient, check cardiac enzymes and other lab results, and repeat ECGs.
Are These ST Changes Due to Acute M.I.? There are several accepted guidelines in use for evaluating ST segments for STEMI. Some are simplified for ease of use, and some are very detailed, taking into consideration the patient’s age and gender. There are ECG features that INCREASE the chances of ST elevation being due to acute M.I. These features include:
· ST elevations are in related leads
· ST segments are flat or convex upward (frowning)
· There are reciprocal ST depressions
· There are associated ECG signs of M.I. such as pathological Q waves and inverted T waves
· J points are higher than 1 mm (females have less STE requirement for M.I. diagnosis) Leads V2 and V3 generally require 2 mm of STE for a STEMI diagnosis.
As we evaluate this ECG, we see that the subtle ST elevations are in related leads (V1 - V3). They are flat (V2 and V3) or convex (V1). There is NO reciprocal depression of the ST segments. There are NO pathological Q waves. T waves are inverted in V1 and flat in Lead III, a non-specific finding. And the J points are minimally elevated at 1 mm or less. By most standard protocols, this ECG does not meet the criteria for acute STEMI. This does NOT rule out the possibility of M.I.
Other Considerations It is worth noting that strictly “normal” R wave progression is not seen in this ECG. Leads V2 through V6 show normal R wave progression. That is, the R waves progressively become proportionately larger, while the S waves regress. V1, however, does not have the morphology expected, a small r wave and a deep S wave. We are not sure if this is a lead placement issue or not. When V1 has abnormalities not shared by V2, we sometimes see similar changes in Lead III, because V1 and Lead III are both oriented toward the heart’s right side. In this ECG, Lead III does not resemble Lead V1. Also, there is a left axis deviation. If no other cause for left axis deviation is readily apparent, the cause is presumed to be LEFT ANTERIOR HEMIBLOCK, also called left anterior fascicular block. LAH is sometimes caused by anterior-septal M.I., with an incidence of about 7-15%.
Ref.:Marriott HJL, Hogan RN. Hemiblock in acute myocardial infarction. Chest.1970; 58: 342–344.
