This ECG is from a 77 year old woman who was brought to the Emergency Department by EMS. She was found to be suffering from sepsis.
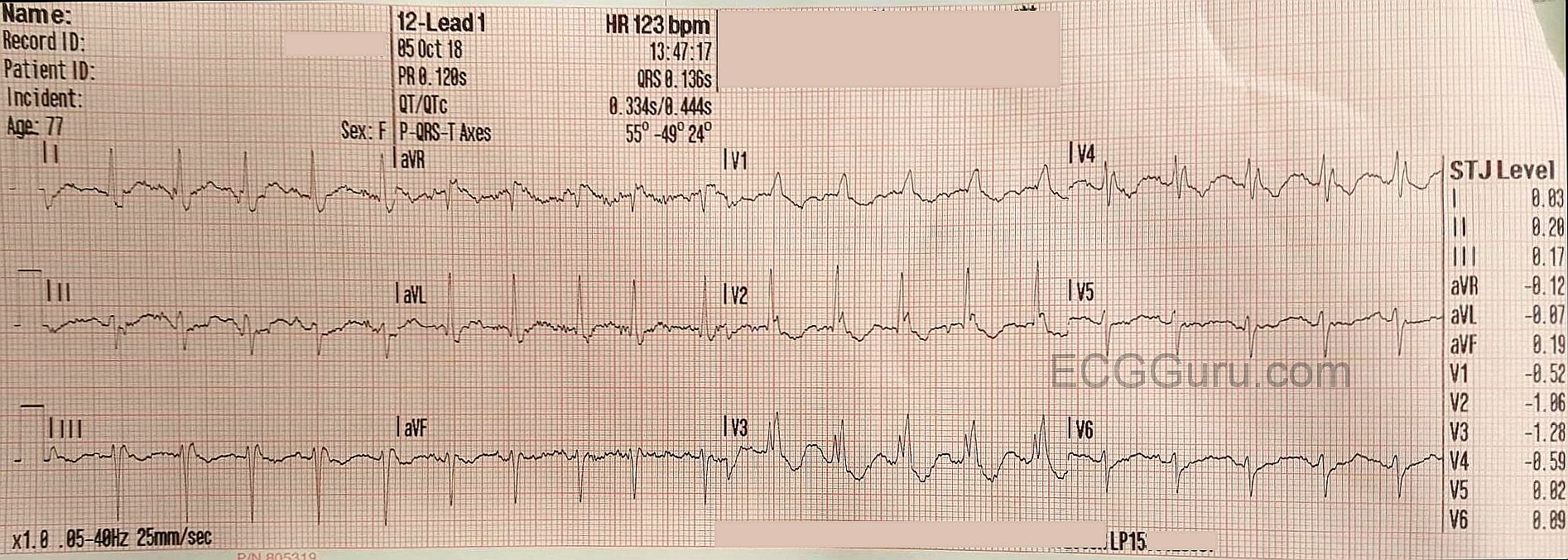
ECG Interpretation The ECG shows the expected sinus tachycardia at 123 beats per minute. There is significant baseline artifact, of the type usually seen with muscle tension. The artifact makes it difficult to assess P waves and PR intervals.
What we do see is RIGHT BUNDLE BRANCH BLOCK and LEFT ANTERIOR HEMIBLOCK, also called LEFTANTERIOR FASCICULAR BLOCK. Together, these are called BIFASCICULAR BLOCK. Most people have three main fascicles in the interventricular conduction system: the right bundle branch and the two branches of the left bundle branch, the anterior-superior fascicle and the posterior-inferior fascicle. In bifascicular block, two of the three are blocked.
The ECG criteria for right bundle branch block are:
* wide QRS (> .12 seconds)
* rSR’ pattern in V1 . (the initial R wave may be hard to see, but the QRS will be predominantly upright.
* wide little S wave in Leads I and V6.
The ECG criteria for left anterior hemiblock are:
* left axis deviation ( between -45 degrees and -90 degrees)
* small q waves in Leads I and aVL
* small r waves with deep S waves in Leads II, III, and aVF.
* delayed intrinsicoid deflection in aVL (the time between the onset of the QRS and the peak of the R wave is greater than .045 seconds).
* increased voltage in the limb leads may cause aVL to meet voltage criteria for left ventricular hypertrophy, but there will be no strain pattern.
Other causes of left axis deviation should be ruled out before diagnosing left anterior hemiblock. For example, the pathological Q waves of advanced inferior wall M.I. can cause left axis deviation, as electrical forces diminish in the damaged tissue.
Most of this ECG’s J points are at or near the baseline, with some ST depression seen in V2 through V4.
Our thanks to Jonathan Hamilton for donating this ECG

